Adherence to antiretroviral therapy (ART) is a significant determinant of viral load suppression in HIV patients. There are inadequate statistical models that bring out the direct effects of ART on the suppression of HIV/AIDS. Traditional regression models address the general determinants of viral load suppression. Regression discontinuity designs, on the other hand, bring out the causal effects of ART on viral load suppression based on various thresholds. This study used the non-parametric fuzzy regression discontinuity design (FRDD) to model viral load suppression in PLWHA. The study began with developing a non-parametric FRDD, simulating the model to assess its performance, and applying the model to the Quality-of-Care dataset from Kaggle. The study focused on viral load suppression as the outcome variable, CD4 count and age as the running variables, gender, and whether a patient received counseling as additional covariates. The optimal thresholds were 40.5 years and 320 cubic millimeters for the CD4. There was an increasing negative treatment effect of ART on viral load suppression as the cutoff points for CD4 count increase. At the same time, there was an increasing negative treatment effect of ART on viral load suppression with increasing age. The compliance ratios for respondents increased with the negative increase in the treatment effect. Other analyses, such as the McCrary density test, bunching test, and manipulation test, indicated that the non-parametric fuzzy regression discontinuity design is effective in modeling viral load suppression.
| Published in | American Journal of Theoretical and Applied Statistics (Volume 13, Issue 5) |
| DOI | 10.11648/j.ajtas.20241305.12 |
| Page(s) | 115-126 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
CD4, Compliance rate, Fuzzy Regression Discontinuity Design, Mccary Test, Viral Load Suppression
Cutoff point | Simulated Dataset | Quality-of-Care Dataset | ||||
|---|---|---|---|---|---|---|
Estimate | Z Value | P value | Estimate | Z Value | P value | |
250 | -53.90 | -1.205 | 0.2281 | -66.18 | -1.35 | 0.178 |
300 | -63.48 | -1.38 | 0.167 | -80.53 | -2.37 | 0.02* |
320 | -86.11 | -1.44 | 0.807 | -106.71 | -2.19 | 0.03* |
400 | -127.86 | -2.374 | 0.017* | -155.29 | -0.89 | 0.37 |
450 | -138.08 | -2.595 | 0.289 | -167.48 | -1.14 | 0.25 |
500 | -164.88 | -2.67 | 0.174 | -177.69 | -2.41 | 0.02* |
Cutoff point | Simulated Dataset | Quality-of-Care Dataset | ||||
|---|---|---|---|---|---|---|
Estimate | Z Value | P value | Estimate | Z Value | P value | |
15 | -0.5587 | -0.406 | 0.685 | -117.3 | -2.505 | 0.01* |
19 | -0.333 | -0.214 | 0.831 | -119.95 | -0.964 | 0.335 |
24 | -0.643 | -0.318 | 0.751 | -124.41 | -1.234 | 0.217 |
32 | -3.108 | -0.827 | 0.408 | -127.72 | -0.107 | 0.914 |
35 | -5.148 | -0.997 | 0.319 | -131.31 | -1.56 | 0.117 |
40.5 | -5.191 | -0.36 | 0.717 | --131.75 | -1.708 | 0.088 |
Cutoff point | Simulated Dataset | Quality-of-Care Dataset | ||
|---|---|---|---|---|
Bandwidth | Observations on the left | Bandwidth | Observations on the left | |
250 | 285.6 | 1505 | 238.82 | 2330 |
300 | 236.9 | 1714 | 496.78 | 2955 |
320 | 355.734 | 1988 | 500.47 | 3153 |
400 | 193.67 | 1267 | 312.14 | 3123 |
450 | 387.34 | 2568 | 392.84 | 3689 |
500 | 135.74 | 655 | 375.19 | 3398 |
Cutoff point | Simulated Dataset | Quality-of-Care Dataset | ||
|---|---|---|---|---|
Bandwidth | Observations on the left | Bandwidth | Observations on the left | |
15 | 3.57 | 105 | 12.48 | 222 |
19 | 3.66 | 203 | 14.40 | 248 |
24 | 3.816 | 367 | 18.201 | 532 |
32 | 3.952 | 607 | 21.94 | 1757 |
35 | 3.68 | 581 | 35.908 | 2449 |
40.5 | 3.60 | 664 | 17.97 | 3421 |
Cutoff point for CD4 Count | Mcrary Test for Simulated Data | McCary test for the Quality-of-Care dataset | Cutoff point for age | Mcrary Test for Simulated Data | McCary test for the Quality-of-Care dataset |
|---|---|---|---|---|---|
250 | 0.986 | 0.4017 | 15 | 0.00012 | - |
300 | 0.622 | 0.7856 | 19 | <0.0000 | <0.000 |
320 | 0.388 | 0.6206 | 24 | <0.0000 | <0.000 |
400 | 0.544 | 0.2545 | 32 | <0.0000 | <0.000 |
450 | 0.185 | 0.0009 | 35 | <0.0000 | <0.000 |
500 | 0.696 | 0.02 | 40.5 | <0.0000 | <0.000 |
AIDS | Acquired Immunodeficiency Syndrome |
ART | Antiretroviral Therapy |
CD4 | Count Cluster of Differentiation 4 Count |
FRDD | Fuzzy Regression Discontinuity Design |
HIV | Human Immunodeficiency Virus |
LATE | Local Average Treatment Effect |
PLWHA | People Living with HIV or AIDS |
| [1] |
Nguyen, M. A Guide on Data Analysis. Bookdown. 2020.
https://bookdown.org/mike/data_analysis/regression-discontinuity.html |
| [2] | Gelman, A., Imbens, G. Why high-order polynomials should not be used in regression discontinuity designs. Journal of Business & Economic Statistics. 2019, 37(3), 447-456. |
| [3] | Dong, F., Zhang, Y., Zhou, Y. Fuzzy regression discontinuity design for causal effect of HIV treatment on viral suppression: A study of China. International Journal of Environmental Research and Public Health. 2021, 18(3), 1072. |
| [4] | Zhang, S., Chen, X., Leng, R. Fuzzy regression discontinuity design in the evaluation of HIV/AIDS intervention. Journal of Biomedical Research. 2019, 33(2), 80-84. |
| [5] | He, Y., Bartalotti, O. Wild bootstrap for fuzzy regression discontinuity designs: obtaining robust bias-corrected confidence intervals. The Econometrics Journal. 2020, 23(2), 211-231. |
| [6] | Mafukidze, P. K., Mwalili, S. M., Mageto, T. A Modification to the Fuzzy Regression Discontinuity Model to Settings with Fuzzy Variables. Open Journal of Statistics. 2022, 12(5), 676-690. |
| [7] | Tymejczyk, O., Brazier, E., Yiannoutsos, C. T., Vinikoor, M., van Lettow, M., Nalugoda, F., IeDEA consortium. Changes in rapid HIV treatment initiation after national “treat all” policy adoption in 6 sub-Saharan African countries: regression discontinuity analysis. PLoS medicine, 2019, 16(6), e1002822. |
| [8] | Sibanda, K., Gundu, T., Whata, A. Assessing the Credibility of South Africa's Anti-Retroviral Treatment (ART) Eligibility Guidelines using Regression Discontinuity Designs. In 2020 2nd International Multidisciplinary Information Technology and Engineering Conference (IMITEC). 2020, 1-5. IEEE. |
| [9] | Chib, S., Greenberg, E., Simoni, A. (2014). Nonparametric bayes analysis of the sharp and fuzzy regression discontinuity designs. Econometric Theory. 2014, 1-53. |
| [10] | Pei, Z., Lee, D. S., Card, D., & Weber, A. Local polynomial order in regression discontinuity designs. Journal of Business & Economic Statistics. 2022, 40(3), 1259-1267. |
| [11] | Malaza, A., Mossong, J., Bärnighausen, T., Viljoen, J., Newell, M. L. Population-based CD4 counts in a rural area in South Africa with high HIV prevalence and high antiretroviral treatment coverage. PloS one. 2013, 8(7), e70126. |
| [12] | Yana, Cahyana., Tukino. Prediction Model for Covid-19 Cases in Indonesia Using Linear Regression and Polynomial Regression Methods. 2023, |
| [13] | Ssebutinde, P., Kyamwanga, I. T., Turyakira, E., Asiimwe, S., & Bajunirwe, F. (2018). Effect of age at initiation of antiretroviral therapy on treatment outcomes; A retrospective cohort study at a large HIV clinic in southwestern Uganda. PLoS One, 13(8), e0201898. |
| [14] | Song, A., Liu, X., Huang, X., Meyers, K., Oh, D. Y., Hou, J., Wu, H. From CD4-based initiation to treating all HIV-infected adults immediately: an evidence-based meta-analysis. Frontiers in immunology. 2023, 9, 212. |
APA Style
Miano, C., Mwalili, S., Malenje, B. (2024). Non-Parametric Fuzzy Regression Discontinuity Design in Modelling Viral Load Suppression Among People Living With HIV/AIDS (PLWHA). American Journal of Theoretical and Applied Statistics, 13(5), 115-126. https://doi.org/10.11648/j.ajtas.20241305.12
ACS Style
Miano, C.; Mwalili, S.; Malenje, B. Non-Parametric Fuzzy Regression Discontinuity Design in Modelling Viral Load Suppression Among People Living With HIV/AIDS (PLWHA). Am. J. Theor. Appl. Stat. 2024, 13(5), 115-126. doi: 10.11648/j.ajtas.20241305.12
AMA Style
Miano C, Mwalili S, Malenje B. Non-Parametric Fuzzy Regression Discontinuity Design in Modelling Viral Load Suppression Among People Living With HIV/AIDS (PLWHA). Am J Theor Appl Stat. 2024;13(5):115-126. doi: 10.11648/j.ajtas.20241305.12
@article{10.11648/j.ajtas.20241305.12,
author = {Caroline Miano and Samuel Mwalili and Bonface Malenje},
title = {Non-Parametric Fuzzy Regression Discontinuity Design in Modelling Viral Load Suppression Among People Living With HIV/AIDS (PLWHA)
},
journal = {American Journal of Theoretical and Applied Statistics},
volume = {13},
number = {5},
pages = {115-126},
doi = {10.11648/j.ajtas.20241305.12},
url = {https://doi.org/10.11648/j.ajtas.20241305.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajtas.20241305.12},
abstract = {Adherence to antiretroviral therapy (ART) is a significant determinant of viral load suppression in HIV patients. There are inadequate statistical models that bring out the direct effects of ART on the suppression of HIV/AIDS. Traditional regression models address the general determinants of viral load suppression. Regression discontinuity designs, on the other hand, bring out the causal effects of ART on viral load suppression based on various thresholds. This study used the non-parametric fuzzy regression discontinuity design (FRDD) to model viral load suppression in PLWHA. The study began with developing a non-parametric FRDD, simulating the model to assess its performance, and applying the model to the Quality-of-Care dataset from Kaggle. The study focused on viral load suppression as the outcome variable, CD4 count and age as the running variables, gender, and whether a patient received counseling as additional covariates. The optimal thresholds were 40.5 years and 320 cubic millimeters for the CD4. There was an increasing negative treatment effect of ART on viral load suppression as the cutoff points for CD4 count increase. At the same time, there was an increasing negative treatment effect of ART on viral load suppression with increasing age. The compliance ratios for respondents increased with the negative increase in the treatment effect. Other analyses, such as the McCrary density test, bunching test, and manipulation test, indicated that the non-parametric fuzzy regression discontinuity design is effective in modeling viral load suppression.
},
year = {2024}
}
TY - JOUR T1 - Non-Parametric Fuzzy Regression Discontinuity Design in Modelling Viral Load Suppression Among People Living With HIV/AIDS (PLWHA) AU - Caroline Miano AU - Samuel Mwalili AU - Bonface Malenje Y1 - 2024/10/10 PY - 2024 N1 - https://doi.org/10.11648/j.ajtas.20241305.12 DO - 10.11648/j.ajtas.20241305.12 T2 - American Journal of Theoretical and Applied Statistics JF - American Journal of Theoretical and Applied Statistics JO - American Journal of Theoretical and Applied Statistics SP - 115 EP - 126 PB - Science Publishing Group SN - 2326-9006 UR - https://doi.org/10.11648/j.ajtas.20241305.12 AB - Adherence to antiretroviral therapy (ART) is a significant determinant of viral load suppression in HIV patients. There are inadequate statistical models that bring out the direct effects of ART on the suppression of HIV/AIDS. Traditional regression models address the general determinants of viral load suppression. Regression discontinuity designs, on the other hand, bring out the causal effects of ART on viral load suppression based on various thresholds. This study used the non-parametric fuzzy regression discontinuity design (FRDD) to model viral load suppression in PLWHA. The study began with developing a non-parametric FRDD, simulating the model to assess its performance, and applying the model to the Quality-of-Care dataset from Kaggle. The study focused on viral load suppression as the outcome variable, CD4 count and age as the running variables, gender, and whether a patient received counseling as additional covariates. The optimal thresholds were 40.5 years and 320 cubic millimeters for the CD4. There was an increasing negative treatment effect of ART on viral load suppression as the cutoff points for CD4 count increase. At the same time, there was an increasing negative treatment effect of ART on viral load suppression with increasing age. The compliance ratios for respondents increased with the negative increase in the treatment effect. Other analyses, such as the McCrary density test, bunching test, and manipulation test, indicated that the non-parametric fuzzy regression discontinuity design is effective in modeling viral load suppression. VL - 13 IS - 5 ER -
Statistics and Actuarial Science, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
Statistics and Actuarial Science, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
Statistics and Actuarial Science, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
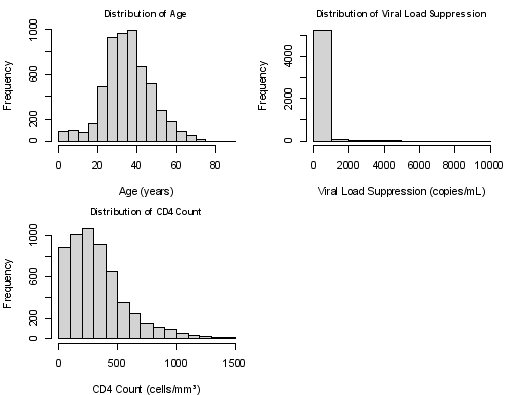
Figure 1. Graphical Representation of the Distributions of the Continuous Variables Used in the Study (Age, CD4 Count, and Viral Load) from the Quality-of-Care Dataset.
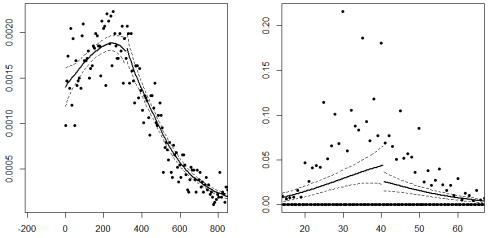
Figure 2. The McCary Density Plot for Discontinuities in CD4 count (RHS) and Age (LHS) for simulated dataset.
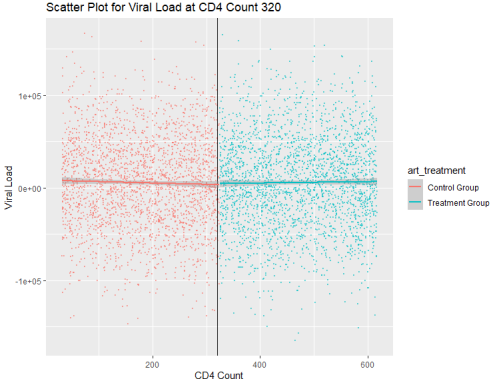
Figure 3. Manipulation Test Graph for CD4 Count.

Figure 4. Manipulation Test Graph for Age.
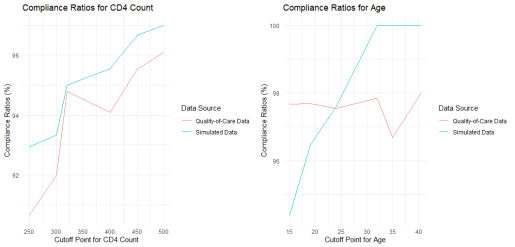
Figure 5. Compliance Ratios
Figure 6. Definitions of Youths by Various entities.
Information

